增强型上肢假肢控制:EMG与NIRS信号融合接口
需积分: 17 13 浏览量
更新于2024-09-07
收藏 1.89MB PDF 举报
本文主要探讨了"肌电(Electromyography, EMG)与近红外光谱(Near-Infrared Spectroscopy, NIRS)信号在上肢假肢控制中的应用与融合"。随着先进肌电假肢的发展,其性能受限于截肢残余肌肉的信号质量和实时控制能力。为了克服这些局限,研究者提出了一种创新的人机交互界面设计,它结合了EMG和NIRS这两种生物信号检测技术。
EMG是通过记录肌肉活动时产生的微弱电流变化来监测肌肉收缩,常用于控制假肢运动。然而,单凭EMG信号可能存在信号干扰、信噪比低等问题,特别是在残余肌肉信号弱或不稳定的情况下。NIRS则是一种非侵入性的光谱技术,可以测量血液中的血红蛋白对特定波长光的吸收变化,从而反映肌肉的氧合状态,提供额外的生理信息。
在这项研究中,作者通过实验比较了三种不同类型的传感器:纯EMG、纯NIRS以及EMG和NIRS相结合的方法。实验包括13名健康志愿者和三名截肢者,他们参与了虚拟假肢运动识别系统的评估。实验结果显示,结合EMG和NIRS的系统在离线分类准确率(Classification Accuracy, CA)和实时性能方面均优于单独使用EMG或NIRS的情况。离线分类准确率的提升表明了多源信号融合有助于更精确地识别和解析肌肉活动;而在线性能的改善则反映了这种融合方法能够提供更稳定和实时的假肢控制。
这项工作对于提升上肢假肢的控制精度和用户体验具有重要意义,因为它展示了如何通过集成多种生物信号技术来增强人机接口,弥补传统肌电信号的不足。未来的研究可能会进一步优化信号处理算法,提高实时性能,并探索更多的应用场景,例如精细动作控制或者适应性反馈。这种结合EMG和NIRS的智能假肢控制系统有望推动假肢技术向着更加自然、高效的方向发展。
566 IEEE TRANSACTIONS ON HUMAN-MACHINE SYSTEMS, VOL. 47, NO. 4, AUGUST 2017
TABLE II
D
EMOGRAPHIC CHARACTERISTICS OF THE THREE AMPUTEE SUBJECTS
Subject ID Gender Age (years) Affected side Residual stump length Cause of amputation Time since amputation Prosthesis usage
A1 Male 37 Right 23 cm Tumor 9 years All day, cosmetic
A2 Male 38 Right 16 cm Traumatic 10 years Half day, myoelectric
A3 Male 62 Left 16 cm Traumatic 9 y ears Half day, cosmetic
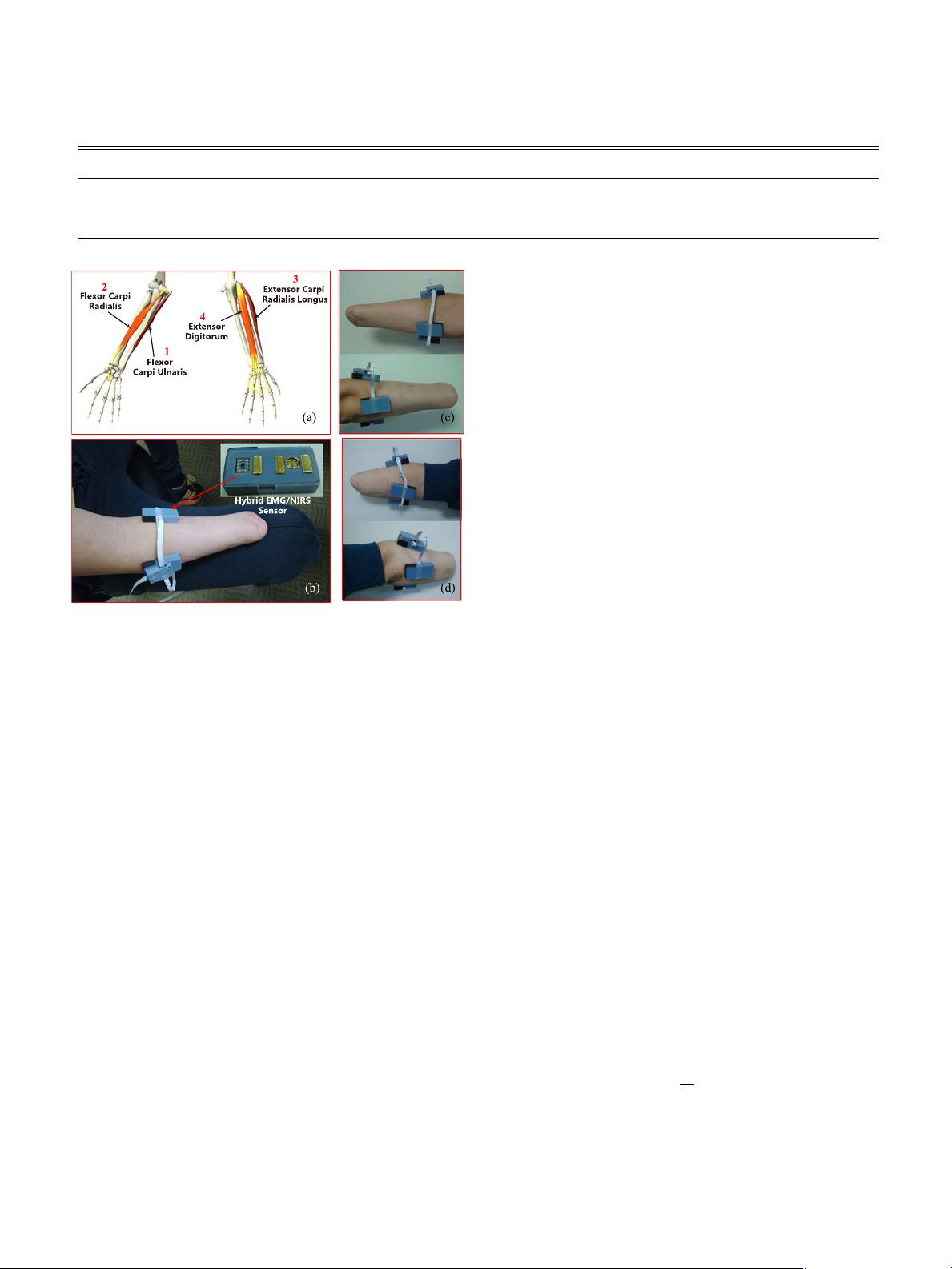
Fig. 2. Placement of hybrid EMG/NIRS sensors. (a) Targeted muscles for
deploying sensors; channels 1 and 2 are attached to FCU and FCR, respectively;
channels 3 and 4 are placed on ECRL and ED, respectively. (b) Sensor placement
of amputee subject A1. Anterior and posterior views of the stump for (c) A1
and (d) A2.
informed consents before the experiment and the procedures
accorded with the declaration of Helsinki.
The experiment included two separate parts. The first part
was for the offline evaluation of the sensor fusion approach that
combined the EMG and NIRS signals. In the second part, the
subjects performed the online Motion Test [11] for assessing the
real-time performance of controlling a virtual prosthetic hand.
Ten of the 13 able-bodied subjects and the three amputee sub-
jects completed the second part, and the time interval between
these two parts ranged from several days to three months.
B. Offline Data Acquisition and Pattern Classification
1) Sensor Placement: For every subject, four hybrid
EMG/NIRS sensors [39] were attached above flexor carpi ul-
naris (FCU), flexor carpi radialis (FCR), extensor carpi ra-
dialis longus (ECRL), and extensor digitorum (ED), respec-
tively, by using double-sided adhesive tapes, as shown in Fig. 2
(skin treatment with alcohol before the attachment). The hybrid
EMG/NIRS sensor integrated a bandpass filter (20–450 Hz) for
an EMG signal and a l ow-pass filter (0–300 Hz) for an NIRS
signal to attenuate the effects of unwanted noises. The EMG
and NIRS signals were amplified with gains of 500 and 1.3,
respectively, and were sampled at 1000 Hz. The near-infrared
light sources contained three wavelengths (730, 805, and 850
nm), and the near-infrared LEDs were switched ON and OFF
sequentially driven by a pulse train so that the detected signals
at each wavelength could be separated. The pulse frequency was
10 Hz, and the duty ratio was 50% [39].
2) Data Acquisition: During the experiments, the subjects
were required to naturally drop down their arms toward the
ground, and the following 13 types of contractions were per-
formed for ten steady-state repetitions: wrist flexion (WF), wrist
extension (WE), radial deviation (RD), ulnar deviation (UD),
pronation (PN), supination (SN), fist (FS), hand open (HO), in-
dex point (IP), fine pinch (FP), tripod grasp (TG), ball grasp
(BG), and rest. These motions were selected as they were fre-
quently encountered in ADL [9]. Each contraction was held for
5 s during a repetition to generate sufficient data for further of-
fline analysis including feature extraction and pattern classifica-
tion, which was widely adopted in similar studies [8], [13], [14].
Self-evaluated moderate contraction was used for all subjects,
and there was a 2-min break between two adjacent repetitions
to avoid muscle fatigue.
3) Feature Extraction: The raw EMG and NIRS data were
segmented into a series of 300-ms windows with an overlap of
200 ms, and features were extracted from these sliding win-
dows, as shown in Fig. 3. The 300-ms analysis window was
adopted for computing the feature vector to reduce the non-
stationary of EMG signals and was exactly matched with the
whole period of NIRS signals. A segment of EMG/NIRS sig-
nals with 300 ms contained enough information to predict a
motion intention. Moreover, the 200-ms overlapping (100 ms of
increment) of the sliding windows was selected to maximally
utilize the computing capacity and produce decision stream as
dense as possible to meet the real-time control requirement [7],
[13]. Four-dimensional EMG time-domain (EMGTD) features
[7] were extracted, namely, mean absolute value (MAV), zero
crossings, slope sign changes, and waveform length (WL). Three
NIRS features were extracted as NIRTD feature set, namely,
MAV, WL, and NIRV (the variance of the NIRS signal), which
were calculated as (1)–(3), respectively. The NIRTD feature set
represents the hemodynamics and blood flow properties during
muscle contractions. A concatenation of EMGTD and NIRTD,
which integrated the information of EMG and NIRS, was de-
noted as combined feature set (EMGTD-NIRTD)
x
mav
=
1
N
N
n=1
|x
n
| (1)
where N is the window size, and x
n
is the NIRS signal
x
wl
=
N
n=2
|x
n
| (2)
剩余11页未读,继续阅读
2021-09-30 上传
2022-12-20 上传
2015-08-10 上传
2023-04-29 上传
2023-07-13 上传
2023-07-01 上传
2023-05-12 上传
2024-03-10 上传
2023-06-11 上传

天空她像什么
- 粉丝: 0
- 资源: 1
 我的内容管理
展开
我的内容管理
展开







最新资源
- 新代数控API接口实现CNC数据采集技术解析
- Java版Window任务管理器的设计与实现
- 响应式网页模板及前端源码合集:HTML、CSS、JS与H5
- 可爱贪吃蛇动画特效的Canvas实现教程
- 微信小程序婚礼邀请函教程
- SOCR UCLA WebGis修改:整合世界银行数据
- BUPT计网课程设计:实现具有中继转发功能的DNS服务器
- C# Winform记事本工具开发教程与功能介绍
- 移动端自适应H5网页模板与前端源码包
- Logadm日志管理工具:创建与删除日志条目的详细指南
- 双日记微信小程序开源项目-百度地图集成
- ThreeJS天空盒素材集锦 35+ 优质效果
- 百度地图Java源码深度解析:GoogleDapper中文翻译与应用
- Linux系统调查工具:BashScripts脚本集合
- Kubernetes v1.20 完整二进制安装指南与脚本
- 百度地图开发java源码-KSYMediaPlayerKit_Android库更新与使用说明
