放射组学:医学影像与精准医疗的桥梁
需积分: 50 199 浏览量
更新于2024-09-07
收藏 4.7MB PDF 举报
"Radiomics: the bridge between medical imaging and personalized medicine"
放射组学,作为医学影像与个性化精准医学之间的桥梁,是一种新兴的技术,它通过从常规医疗成像中提取大量定量图像特征,来提升临床诊断、预后评估和治疗预测的准确性。在癌症研究中,放射组学扮演着越来越关键的角色。这项技术依赖于先进的图像分析工具和快速的数据处理,旨在通过图像特征(即基于图像的签名)实现精确的疾病诊断和疗法定制。
放射组学的工作流程主要包括以下几个步骤:首先,对数字化的医学图像进行识别,从中提取大量的定量特征;其次,将这些特征数据存储在联合数据库中,便于统一管理和分析;最后,通过对这些高维数据的挖掘,提取出有价值的信息,用于临床决策支持系统(CDSS),以辅助医生做出更精准的医疗决策。
放射组学的发展受益于计算机辅助诊断、预测和治疗的研究历史,但同时也面临着一些挑战。目前,由于该领域的迅速发展,很多已发表的研究在科学完整性及临床相关性的标准化评估上存在不足。因此,建立严格的方法学评估标准和报告指南是放射组学成熟为一门学科的必要条件。
深度学习作为人工智能的一个分支,已经在医学影像分析中展现出巨大的潜力,特别是在放射组学中。通过深度神经网络,可以自动学习和理解图像中的复杂模式,进一步提升特征提取的效率和准确性。这使得放射组学能够从海量的图像数据中发现潜在的生物标记物,为癌症患者提供个性化的治疗方案。
尽管放射组学带来了许多机遇,如提高肿瘤病理生理学的理解,促进精准医疗的发展,但它也存在一些问题。例如,数据的标准化、特征选择的最优策略、模型的可重复性和解释性等都是当前研究的重点。此外,保护患者隐私和确保数据安全也是放射组学广泛应用时必须考虑的关键因素。
放射组学正在逐步成为连接医学影像和个性化医疗的重要纽带。通过持续的科研进步和技术优化,有望克服现有挑战,实现从影像到治疗决策的全面个性化,从而提高医疗质量和患者生存率。
Nature Reviews | Clinical Oncology
Cardiac CT Radiomics MACE Analysis
Phantom studies
An artificial structure that
imitates human tissue
properties is scanned on
multiple machines to
characterize scan output
against a known physical
standard.
comparability of radiomic studies can be achieved only
by extensive disclosure of imaging protocols. We wish
to emphasize this point, and provide examples of how
protocols should be reported in future radiomics studies
(Supplementary informationS1).
Medical imaging
Segmentation. VOIs are segmented manually or (semi-)
automatically
19
. This segmentation determines which vox-
els within an image are analysed, thus, the variability in seg-
mentation can introduce bias in the evaluation of derived
radiomic features
20
. Multiple-segmentation is a method to
limit the extent of this bias. Examples that enable robust
features to be observed
21
include: evaluation by multiple
clinicians, perturb segmentations with noise, combination
of diverse algorithms, or use different stages of the breath-
ing cycle. Key considerations are how the segmentation was
performed, and how sensitive the radiomics analysis is to
different segmentation methods
22
. For example, a semi-
automatic segmentation method can result in different
radiomic features than a manual delineation.
Phantom studies. The determination of inter-scanner and
inter-vendor variability of features is important in radi-
omics
23
. In cases in which radiomic studies rely on data
from multiple scanners, neglecting this variability can
jeopardize the analysis of studies—that is, the proposed
radiomic-based prediction model might not perform ade-
quately on external datasets if new data are acquired on
different scanners. As data from patients scanned on mul-
tiple devices is scarce and subject to uncertainties (such as
organ motion, or different imaging protocols), phantom
studies are a suitable means to gauge these uncertainties
and identify features that rely on the vendor. In essence,
phantom studies provide a risk-mitigation strategy to help
navigate from the current clinical imaging scenario to the
desired optimal imaging scenario.
Imaging at multiple time points. Additional sources
of variability in radiomics features are organ motion or
expansion or shrinkage of the target volume. Radiomics
features that are strongly dependent on these factors can
have limited applicability. To account for these sources of
variability, available test-retest data
24–26
can be exploited
to measure radiomics feature stability. For example, two
datasets of images acquired within a small period of time
from a patientcohort.
Feature extraction
The essence of radiomics is the high-throughput extrac-
tion of quantitative image features to characterize VOIs.
Feature values are dependent upon factors that can
include image pre-processing (for example, filtering, or
intensity discretization) and reconstruction (for exam-
ple, filtered back projection, or iterative reconstruction).
Furthermore, variation exists in feature nomenclature,
mathematical definition, methodology, and software
implementation of the applied feature extraction
algorithms
27–29
. In order to facilitate inter- operability
of radiomic features, differences in nomenclature,
algorithms, software implementations, as well as other
methodological aspects must be elucidated.
Exploratory analysis
Radiomic and non-radiomic features should be com-
bined with the prediction target to create a single
dataset. This approach enables the investigation of
relationships between features. Groups of highly cor-
related radiomics features can be identified via clus-
tering, and these features can be reduced to single
archetypal features per cluster. Radiomic features that
are well-correlated with routine clinical features (such
as tumour stage) do not provide additional information.
Auxiliary feature data collected from multiple segmen-
tations, multiple imaging, and phantom studies, can be
exploited to assess feature robustness. Volatile or robust
features can be identified and subsequently excluded
from model development. For example, a feature that
is robust for the prediction of overall survival for lung
cancer (that is, imaged and segmented in a certain way)
for a given dataset could be volatile for the prediction of
pneumonitis in lung cancer (imaged and segmented in
an alternative way) for a given dataset. Thus, the pro-
cess of feature reduction and/or exclusion should be
described clearly.
Modelling
Radiomic modelling involves three major aspects: fea-
ture selection, modelling methodology, and validation.
Feature selection should be data-driven owing to the
vast in- human range of possible radiomics features; such
analysis should be performed in a robust and transparent
manner. To achieve holistic models, features beyond radi-
omics (such as data from clinical records, data obtained
during treatment or biological and/or genetic) should
also be incorporated. Regarding the choice of modelling
methodology, the identification of optimal machine-
learning methods for radiomic applications is a crucial
step towards stable and clinically relevant CDSS; thus, in
the ideal scenario, multiple machine-learning methods
should be employed
30
and the implementation should be
comprehensively documented. A non-validated model is
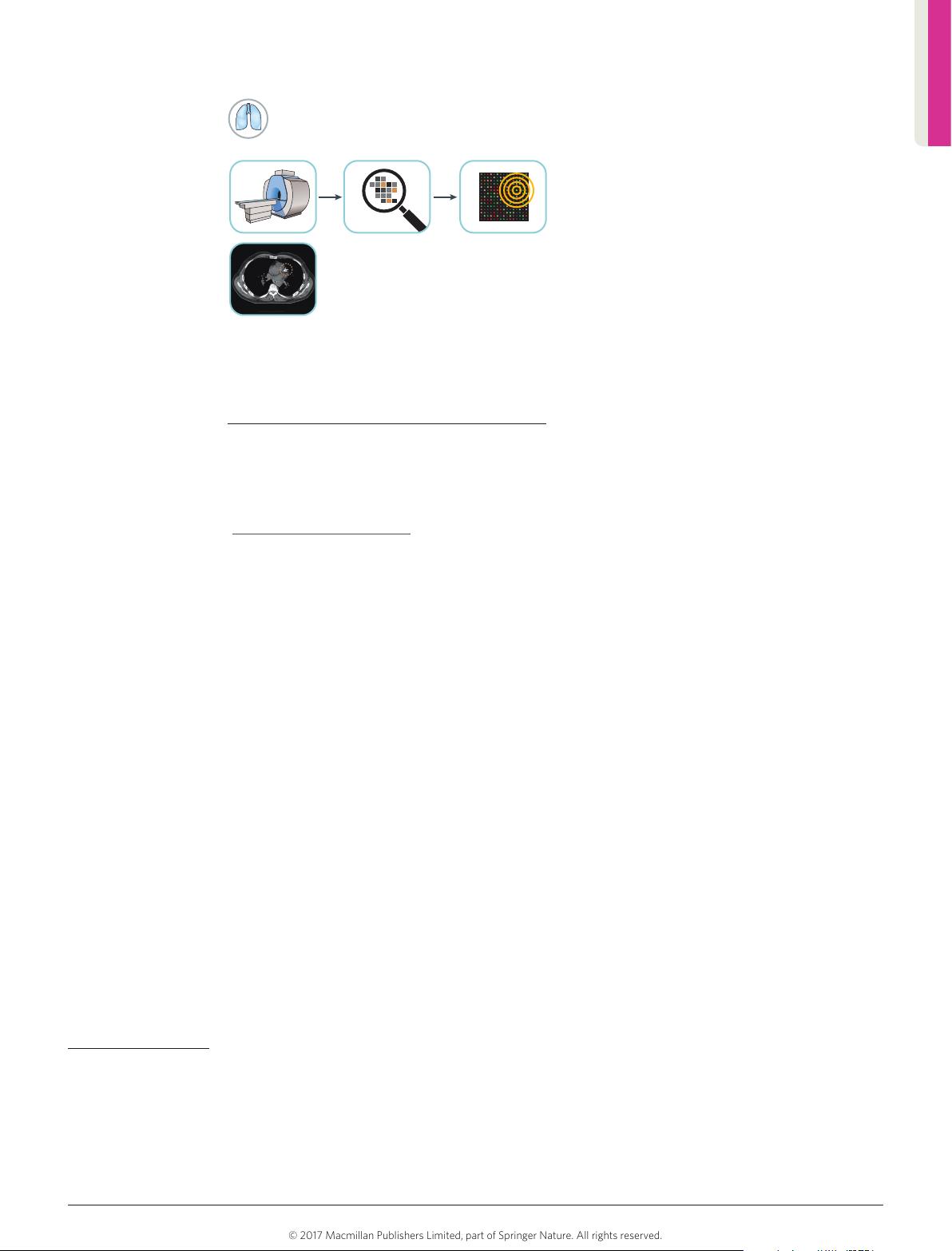
Figure 2
|
Radiomics in cardiology. The current gold standard
for quantification of coronary calcifications visible on CT is the
‘Agatston’ method (based upon intensity and volume).
Radiomic features can improve quantification, differentiation
between calcified and non-calcified plaques, and thus the
prediction of Major Adverse Cardiac Events (MACE).
REVIEWS
NATURE REVIEWS
|
CLINICAL ONCOLOGY VOLUME 14
|
DECEMBER 2017
|
751
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
剩余13页未读,继续阅读
1600 浏览量
102 浏览量
247 浏览量
2021-09-25 上传
236 浏览量
2021-07-10 上传
2023-06-08 上传
138 浏览量
239 浏览量
108 浏览量

HAO亮
- 粉丝: 558
 我的内容管理
展开
我的内容管理
展开







最新资源
- 网页自动刷新工具 v1.1 - 自定义时间间隔与关机
- pt-1.4协程源码深度解析
- EP4CE6E22C8芯片三相正弦波发生器设计与实现
- 高效处理超大XML文件的查看工具介绍
- 64K极限挑战:国际程序设计大赛优秀3D作品展
- ENVI软件全面应用教程指南
- 学生档案管理系统设计与开发
- 网络伪书:社区驱动的在线音乐制图平台
- Lettuce 5.0.3中文API文档完整包下载指南
- 雅虎通Yahoo! Messenger v0.8.115即时聊天功能详解
- 将Android手机转变为IP监控摄像机
- PLSQL入门教程:变量声明与程序交互
- 掌握.NET三层架构:实例学习与源码解析
- WPF中Devexpress GridControl分组功能实例分析
- H3Viewer: VS2010专用高效帮助文档查看工具
- STM32CubeMX LED与按键初始化及外部中断处理教程
