医学影像系统技术:成像模式与计算机辅助诊断
"Medical Imaging Systems Technology - Modalities" 是一本由Cornelius T Leondes编辑的五卷系列书籍中的一卷,专注于医学成像系统的各种技术,即成像方式。该系列作为一本重要的参考工作(Major Reference Work),全面探讨了医学成像领域的关键主题,每卷书都集中于一个特定的、基础性的重要领域。
这本关于“Modalities”的卷,详细介绍了诸如计算机断层扫描(CT)、磁共振成像(MRI)等新型成像技术,这些技术结合强大的计算能力,极大地提高了医疗诊断的准确性和效率,从而拯救了许多患者的生命,并改善了我们所有人的生活质量。书中涵盖了国际上领先专家的贡献,旨在为医学、技术以及计算机科学领域的专业人士提供深入的见解和知识。
医学成像系统技术的发展促进了跨学科的合作,使得同时拥有物理学、计算机科学博士学位和医学学位的年轻医生群体迅速壮大。这些医生和技术专家的技能在这一具有重大意义的领域中发挥了关键作用。
书中涉及的内容可能包括但不限于:成像原理、图像处理方法(如机器视觉)、不同成像模式的比较、数据采集与重建算法、图像分析与解释、以及这些技术在临床实践中的应用案例。此外,还可能讨论了技术的进步如何影响诊断决策优化,特别是在心血管和大脑系统方面的成像方法。
这本书对于理解医学成像技术的最新发展和应用至关重要,无论是对医学专业人员,还是对希望深入研究医学成像技术的科研工作者和工程技术人员,都是宝贵的参考资料。书中强调了尊重版权的重要性,未经许可,任何部分都不能以任何形式复制或通过任何电子或机械方式传播,包括但不限于影印、录音或任何现有的或未来的信息存储和检索系统。
“Medical Imaging Systems Technology - Modalities”是医学成像领域的权威之作,它详细地阐述了各种成像技术的原理、应用和对未来医学实践的影响。
Multislice Helical Computed Tomography 7
2.1. CT Angiography
CT Angiography (CTA) is the clinical application that has benefited most from the
imaging speed improvements afforded by multislice scanners.
8
CTA involves the
imaging of the vessels of the trunk, brain, or extremities after intravenous injection
of an iodinated contrast bolus. Imaging is performed after waiting for the bolus to
travel through the heart into the arteries. Because the distribution of the contrast
agent changes constantly, the speed of imaging largely determines the resulting
image quality. Multislice CT technology even makes it possible to perform bolus
tracking: Following the bolus of contrast as it travels through the body, even over
the distance from the heart to the feet that is traversed in just a few seconds in a
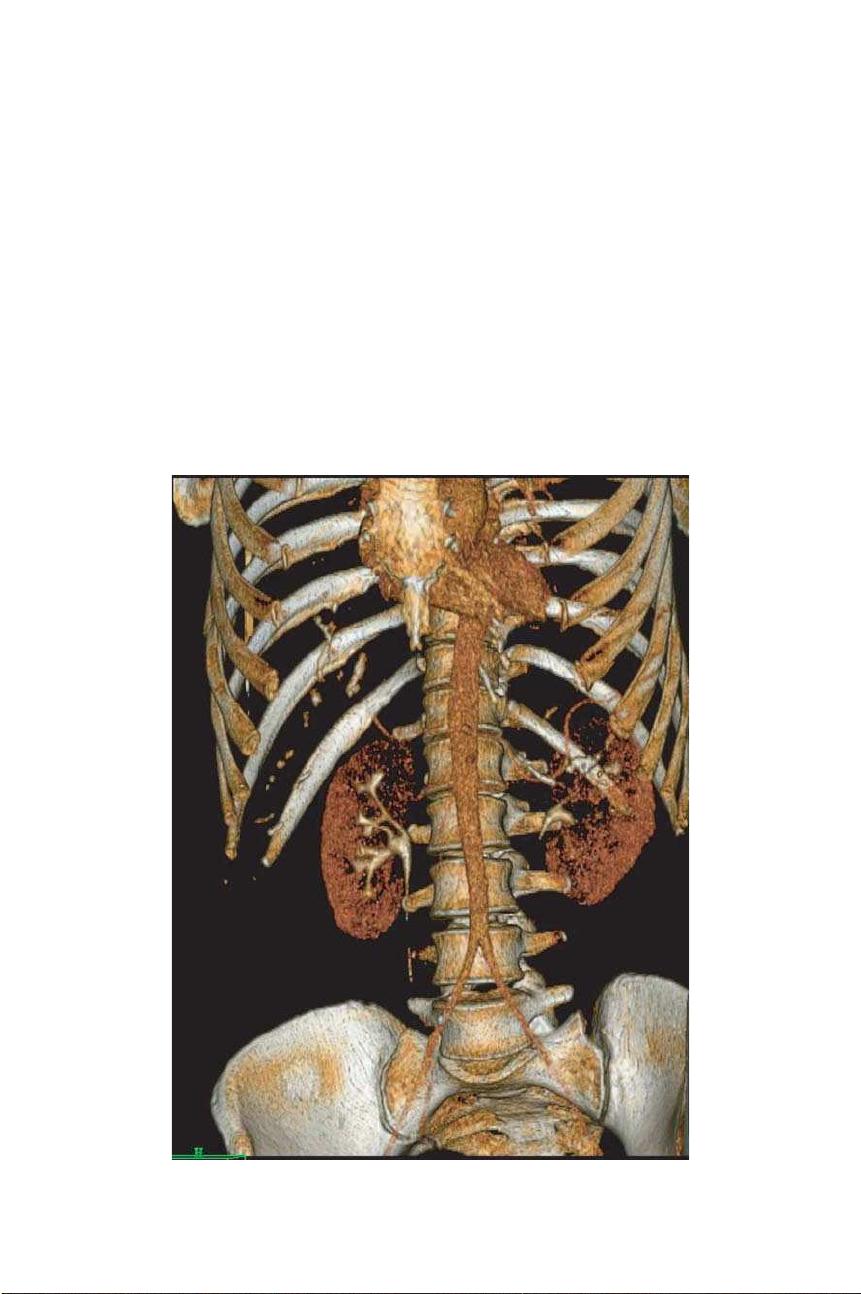
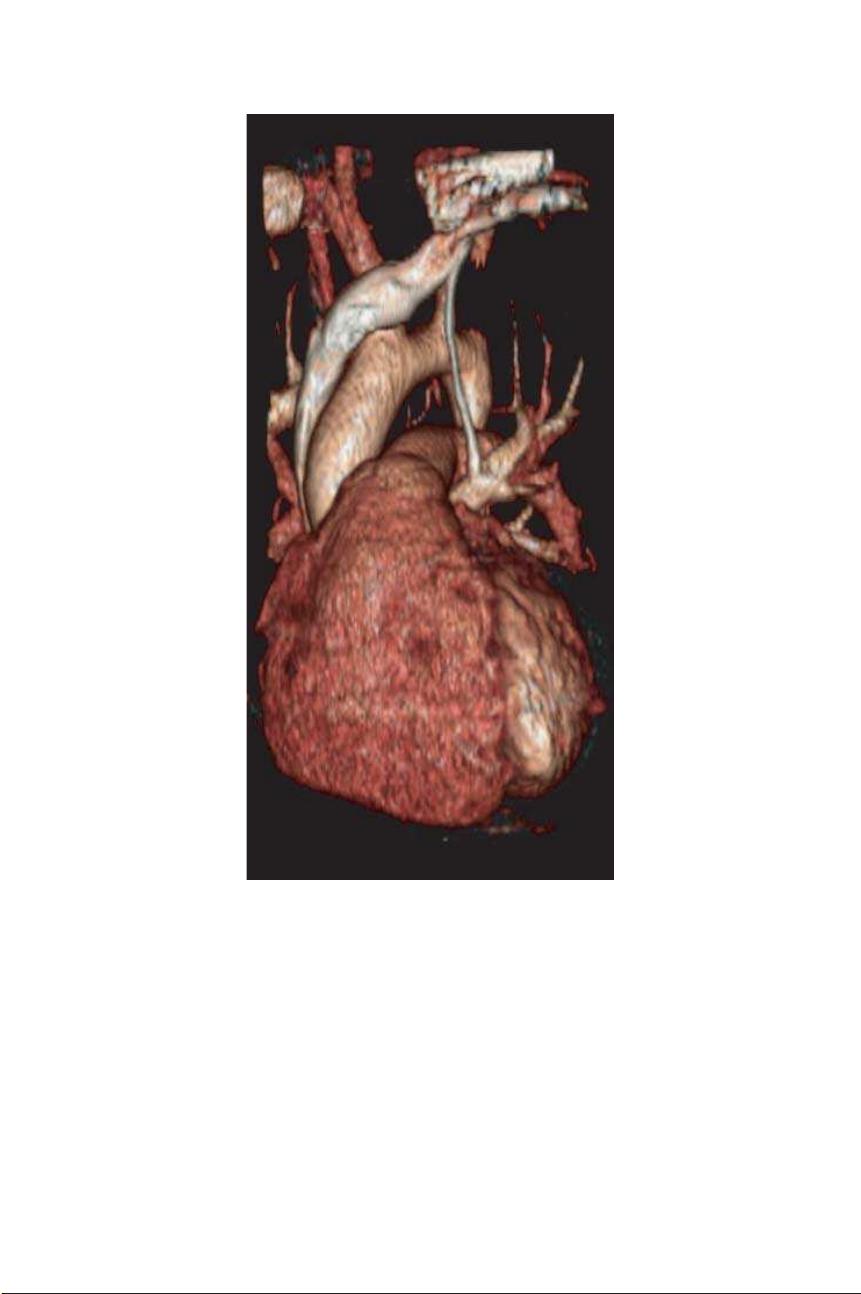
runoff study. A volume rendering of a CTA study conducted on a 40- slice scanner
is shown in Fig. 4.
Fig. 4. Volume rendering of a CT angiography study showing bones, vessels, and enhanced
organs. The study was performed on a Philips Brilliance 40 CT scanner.



剩余362页未读,继续阅读
2021-12-01 上传
549 浏览量
2021-10-01 上传
114 浏览量
193 浏览量
209 浏览量
568 浏览量
2023-05-12 上传
2023-06-06 上传

hh1021
- 粉丝: 0
- 资源: 7
 我的内容管理
展开
我的内容管理
展开







